
1. INTRODUCTION
Asherman syndrome is caused by endometrial basal layer injury or infection, which leads to uterine cavity fibrosis and adhesion, resulting in dysmenorrhea, infertility, and pregnancy loss [1,2]. Damage caused by overly aggressive curettage, infection, or surgical manipulation of the basalis layer comprises the majority of these cases. This causes regenerative process dysfunction, resulting in abnormal endometrial morphology and loss of uterine function. Many studies have attempted to recover the structure and function of the endometrium [3]. The most commonly used therapies are hormones and physical therapy to overcome the adhesions [4]. Although these methods were somewhat effective, many issues made the treatment unsatisfactory. Therefore, more effective and safe procedures should be investigated for improving the endometrium regeneration.
Different from platelet-rich plasma (PRP) and platelet-rich fibrin (PRF) is easy to obtain and does not require any biochemical processing beforehand. Alveolar socket repair in dentistry, regeneration of periodontal defects in healing gingival lesions, facial defects, and scars in plastic surgery are only some of the many applications where PRF has shown success since it is a reservoir of growth factors and contains a substantial quantity of blood cells [5-7]. There are two forms of PRF: Pure PRF and Leukocyte PRF (L-PRF), which are distinguished by the relative abundance of leukocytes in the fibrin matrix [8]. In addition, leukocytes in L-PRF, such as neutrophils and macrophages, have been demonstrated to have a significant role in immunology and to produce substantial amounts of vascular endothelial growth factor (VEGF), which plays a vital part in the mechanism of angiogenesis and tissue regeneration [9,10]. In addition, gel PRF (gPRF) structure has been proved to have a stable matrix and slowly released growth factors, which play a critical role in regenerative medicine [11,12]. However, few studies have been conducted on using PRF to treat damaged endometrium.
The goal of this study was to see if one dose of gPRF could improve damaged endometrium and increase endometrial receptivity in the Asherman’s mouse model.
2. MATERIALS AND METHODS
2.1. Experimental Animals
A 10–12 week-old Mus musculus Var. Albino mice were purchased from Pasteur Institute, Ho Chi Minh City, Viet Nam. Female mice that had given birth were used for this research. Mice were housed in 4–5 per cage with 1107 cm2 of floor space and sustained in the room with 12 h of light/dark cycle, and the condition was 25 ± 3°C at the Laboratory of Tissue Engineering and Biomedical Materials (University of Science, Viet Nam National University at Ho Chi Minh City). Animal methods in this research were accepted by the ethics committee of the University of Science (580B/KHTN-ACUCUS). Female mice’s estrus cycle stage was determined before the experiments.
2.2. Preparation of Mouse gPRF
Using a heart puncture, whole blood was taken from the test mice and placed in the sterile tube without anticoagulant. This experimental tube was centrifuged at 2500 rpm for 15 min (EBA 200, Hettich, Germany). Then, a clot of fibrin was collected in the tube’s center between the red blood cells and the plasma. Forceps were used to grasp the gPRF, and then scissors were used to cut it away from the RBCs. By subtracting the results of the first and second centrifugation steps, we were able to infer the platelet concentration of the gPRF.
2.3. Evaluation of Structure of the PRF
To examine its finer details in two and three dimensions, the gPRF scaffold was fixed in 10% formaldehyde (Merck, Germany) for 24 h and then stained with hematoxyline and eosin (H and E) (Thermo Scientific, USA). Under an inverted microscope, the sample was analyzed (Olympus, Japan). Moreover, scanning electron microscopy (SEM) was utilized to look at the PRF clot’s three-dimensional structure (S-4800, Hitachi, Japan).
2.4. Cultured Mouse Bone Marrow Cells (mBMCs) In Vitro
The mBMCs were provided by the Laboratory of Tissue Engineering and Biomedical Materials. The mBMCs were grown in Dulbecco′s modified Eagle’s medium (DMEM)/nutrient mixture F-12 Ham (Sigma-Aldrich, USA) supplemented with 10% Fetal Bovine Serum (Sigma-Aldrich, USA), 100 U/mL Penicillin and 100 mg/mL Streptomycin (Sigma-Aldrich, USA). This cultural medium was called a complete medium (CM).
2.5. Preparation of Liquid Extract of PRF for In Vitro Experiment
The gPRF was immersed in 10 mL of DMEM/F12 with serum for in vitro cytotoxicity at 37°C, 5% CO2 [13]. The liquid extract of gPRF was kept at 4°C before use.
2.6. In Vitro Cytotoxicity Testing
mBMCs were cultured on a 96 well-plate at 37°C, 5% CO2 until they reached 80% confluence at a cell density of 1.5 × 104 cells per well. The next day, the culture medium was swapped out for one containing either the liquid extract of PRF (the test group), the CM (the blank group), or the latex liquid extract (the positive group). The latex sample measuring 3 × 2 cm was submerged in 1 mL of CM for 24 h to obtain the latex extract [14]. For an additional 24 h, the cells were grown in culture. Finally, the media were replaced with 5 mg/mL MTT (Sigma-Aldrich, USA) and the plate was incubated at 37°C, 5% CO2 for 4 h. The MTT crystals were soluble in a mixture of DMSO (Sigma-Aldrich, USA) and Ethanol (at a rate of 1:1). (Merck, Germany). The volume of formazan product, as quantified by the amount of 490 nm absorbance (Ez Read 400, Biochrom, USA), is directly proportionate to the number of surviving cells. The relative cell viability (%) related to wells, including cell culture medium with liquid extract of PRF and the CM as a vehicle, was evaluated by [A] PRF group/[A] CM group ×100.
2.7. Cell Migration Testing
mBMCs were grown in a 6 well-plate with a density of 105 cells/plate by the CM at 37°C, 5% CO2 to obtain a confluent monolayer. The cells experienced serum starvation for 24 h with a serum-free media (M-). After 1 day, the straight-line scratch is introduced into the cells by using a sterile pipette tip. After the scratch, the plate was gently rinsed with saline to clear away detached cells. The CM, M-, and liquid extract of PRF gel were replenished. By comparing the images at time (0 h) and 24 h, the distance of each gap closure was captured by an inverted microscope (Olympus, Japan) and analyzed by Image J.
2.8. Animal Model and gPRF Treatment
Mice were divided into three groups: The sham group (the control group, n = 6), the negative control group (PBS group, n = 6), and the treated gPRF group (gPRF group, n = 6). Female mice were used to make a murine model according to a published protocol, with an adjustment [15]. Unlike previous research, this experiment was performed on female mice that had been given a litter of pups to remove the primary infertility issue. Briefly, mice were put under anesthesia with ketamine (100 mg/mL, Ilium, Australia), xylazine (20 mg/mL, Ilium, Australia), and saline. After 16 h of injecting with hCG 50 IU/mL (LG Life Science, Korea), the surgery made an incision down the 0.5-cm length of the abdominal wall, cutting through the muscle layer to expose two uterine horns. A 25-gauge needle (25G) was inserted into the lumen, rotated, and withdrawn 4 times to injure two uterine horns. Fragments in the lumen were carefully discarded with saline [15]. The sham group of animals received no injured uterine or gPRF treatment. At the diestrus of the third estrus cycle after induced-damage uterus, a volume of tiny pieces of gPRF (20 μL per horn) was injected into two uterine horns of mice through the vagina. At the fifth estrus cycle, the function of the uterus was determined after receiving gPRF, the treated female mice were bred with fertile males. The vaginal plug found the next morning was counted as day 0 of pregnancy. Then all the male mice were separated. All female mice were sacrificed on day 6, fetuses were counted and embryo development was photographed [16,17].
Besides, the tissues of the uterine horns used to inject gPRF were collected at the pro-estrus period of the fourth estrus cycle. The samples were formaldehyde-fixed (Merck, Germany) for 24 h before being dying H and E. Images were taken under an inverted microscope (Olympus, Japan). The shape and structure of the lumen epithelial cells, as well as the glandular epithelium (subnuclear vacuoles), were morphological criteria. The secretory state of the uterus was assessed. ImageJ 1.8.0 172 was used to calculate the lumen area (LA), endometrial area (EA), and total horn area (THA) of the uterus. The proportion of regenerated endometrium thickness was indirectly estimated by the evaluation of three different ratios, such as the EA to ratio THA, the LA to THA ratio, and the EA to LA ratio.
2.9. Analytical Statistics
Data are expressed as mean ± standard deviation and analyzed with GraphPad Prism 8. P < 0.05 was considered statistically significant.
3. RESULTS
3.1. Preparation of Mouse gPRF
The centrifugation was used to collect the PRF [Figure 1a and b]. The platelet count in the PRF and the original sample was 5.018 ± 1.471 × 109 platelets/mL (P < 0.05) and 0.876 ± 0.164 × 109 platelets/mL, while the mean leukocyte concentration was 0.023 ± 0.012 × 109 leukocytes/mL (P > 0.05) in the PRF and 0.004 ± 0.001 × 109 leukocytes/mL in peripheral blood [Figure 1c and d]. As a consequence, in PRF, the number of platelets was 5 times higher than in normal blood (P < 0.05), but the number of leukocytes had few changes.
 | Figure 1: Gel PRF preparation and the number of blood cells in PRF. (a) The tube underwent the centrifugation; (b) The gel PRF; (c) The number of platelets in PRF (n = 3); (d) The number of leukocytes in PRF (n =3). P < 0.01 (**); P < 0.05 (*); not significant (ns). [Click here to view] |
3.2. Evaluation of Structure of the gPRF
The PRF — was collected after the ankle centrifugation — had dense fibrin with uniform distribution. Furthermore, at the interface between the erythrocyte segment and the fibrin clot, SEM images of gPRF showed platelets trapped in the fibrin network [Figure 2]. As a consequence, platelets accumulated in the lower part of the PRF.
 | Figure 2: The structure of gel PRF. (a) Two dimensions of PRF stained with Hematoxyline and Eosin (H and E) under inverted microscope (Scale bar: 100 μm); (b) Three dimensions of PRF under Scanning Electron Microscope (Scale bar: 10 μm); White arrows: platelets. [Click here to view] |
3.3. In Vitro Cytotoxicity Testing
The relative cell viability (%) of the group exposed to gPRF was 100.3% ± 24.6, while that of the group exposed to CM was 100.0% ± 20.4. The differences between the two sets of numbers are not particularly noteworthy. This percentage, on the other hand, accounted for only 11.44% ± 1.0 of the latex extract medium. When compared side by side, the PRF and the latex extracts displayed statistically significant differences (P < 0.05) [Figure 3]. In conclusion, the in vitro toxicity test demonstrated that PRF gel is not a toxic material.
 | Figure 3: The relative cell viability (%) of mouse bone marrow cells (n = 3). CM: the complete media. P < 0.01 (**); not significant (ns). [Click here to view] |
3.4. Cell Migration Testing
A scratch wound assay was used to examine the effect of gPRF on the ability of cells to migrate following a 24-h incubation [Figure 4]. When the serum-free medium (M-) was used as a negative control, a small proportion of cells migrated into the gap, and the proportion of the acellular blank dropped to 78.59% ± 4.16. In contrast, the gPRF and the CM as the control were considerably reduced to 53.27% ± 15.22 and 56.76% ± 1.97 (P < 0.05), respectively [Figure 5]. Based on the above findings, it was determined that PRF could stimulate bone marrow cells to fill the empty space.
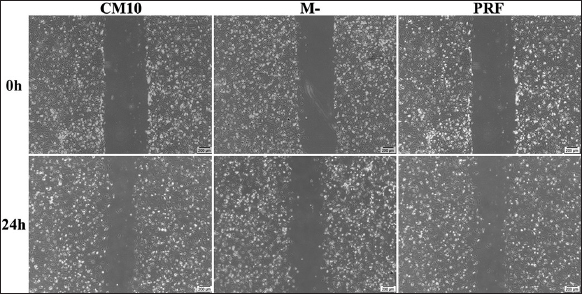 | Figure 4: Migration of mouse bone marrow cells (mBMCs) in 3 types of medium after 0 and 24 h. The images were taken by inverted microscope and the gap was measured by Image J software. M-: free-serum media; CM: complete media. Scale bar: 200 μm. [Click here to view] |
 | Figure 5: The proportion of gap region (n = 3). M-: free-serum media; CM: complete media; P < 0.05 (*). [Click here to view] |
3.5. Animal Model and gPRF Treatment
Following the D0, a 25-gauge needle was used to injure the uterine structure. After three estrus cycles, adhesion was formed in the uterus, yet the regeneration process after injury continued [Figure 6]. In both qualitative and quantitative aspects, endometrial anatomy and function are used to indicate endometrial regeneration.
 | Figure 6: Adhesion was formed after three estrus cycle (n = 3). (a) The uterus after injury (Scale bar: 200 μm); (b) Adhesion in the uterus at ×4 (Scale bar: 200 μm); (c) Adhesion in the uterus at ×40 (Scale bar: 20 μm);Yellow square: adhesion was formed with the injured endometrial basal layer; Scale bar: 200 μm. [Click here to view] |
Qualitatively, histological images showed that there was restoration of endothelial structure after injury in both groups, including the treatment group with gPRF and the non-treated group (PBS infusion). The histological structure of the sham group was similar [Figures 7a-c]. The evidence was that a two-layer structure (basal layer and functional layer covered by epithelium) was observed in these groups. In contrast to the negative control group (PBS), the remaining two groups had subnuclear vacuoles in gland epithelial cells and the appearance of a pseudostratified columnar epithelium. In addition, the uterine gland shape was enlarged and exudate was observed in both the sham group and the treated gPRF group. This phenomenon was not observed in the negative control group (PBS) [Figures 7d-f].
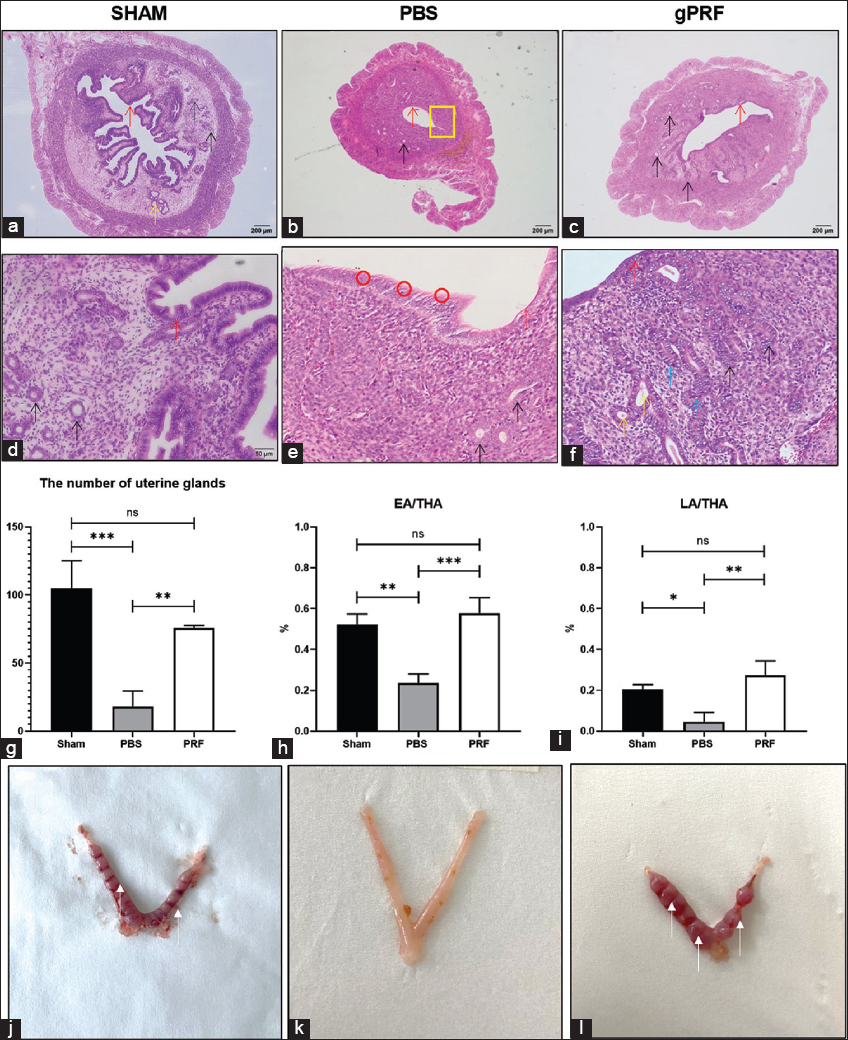 | Figure 7: Changes in the number of glands, shape, and function of the endometrium before and after gPRF administration in three separate groups. (a), (d), and (j): The sham (control) group (n = 3) ; (b), (e) and (k): The PBS (untreated) group; (c), (f) and (l): The gPRF (treated) group; (g): The number of uterine glands of three groups (n =3); (h): The ratio of endometrial area of three groups (n = 3); (i): The ratio of lumen area of three groups. The tissue (Scale bar: 200 μm and 50 μm) and mouse’s uterus after gPRF treatment. White arrow: fetuses; Red arrow: epithelial endometrium; Black arrow: endometrial glands; Yellow arrow: exudate in uterine gland; Blue arrow: paracellular space; Red circle: microvilli; Yellow square: adhesion in uterus. EA/THA: endometrial area/total horn area ratio; LA/THA: lumen area/total horn area ratio. P < 0.001 (***); P < 0.01 (**); P < 0.05 (*); not significant (ns). [Click here to view] |
The number of uterine glands in the sham (control) group, the negative control group (PBS), and the treated gPRF group were 104.7 ± 20.55, 18.00 ± 11.53, and 131.00 ± 39.69, respectively [Figures 7g-i]. There was a significant difference between the gPRF and PBS group (P < 0.05) and there was no significant difference between the gPRF and the sham group. Furthermore, when compared to the other two groups, H and E staining of the mouse uterus in the untreated group (PBS group) revealed that the mice had a small lumen and adhesion.
On the one hand, the percentage of EA/THA in the sham group and in the gPRF group was 0.52 ± 0.05 and 0.58 ± 0.08, while this rate in the PBS group was just 0.24 ± 0.04 (P < 0.05). The percentage of LA/THA in the sham group and in the gPRF group was 0.20 ± 0.02 and 0.27 ± 0.07 compared with the PBS group was 0.04 ± 0.05 (P < 0.05) [Figures 7g-i].
On the other hand, the fetuses were 8.67 ± 3.21 in the gPRF-treated group, 11.67 ± 3.06 in sham group (P > 0.05), and there was no fetus in the PBS group (P < 0.05) at the same time of evaluation. The results indicated that gPRF had a positive effect on damaged uterus [Figures 7j-l].
4. DISCUSSION
In 2001, PRF was first introduced as the next generation of platelet concentration by Choukroun [18]. PRF is prepared by the simplest centrifugation of autologous blood without artificial chemicals or activators [18]. PRF contains large amounts of platelets; therefore, it has various growth factors: VEGF, TGF, PDGF, EGF, and FGF, which have been proven to stimulate endometrial growth [19].
Following the published studies on human PRF, PRF was obtained from mice by performing a single centrifugation step [20]. While the number of leukocytes remained relatively constant, our concentration of platelets showed that the quantity of platelets in mouse PRF was 5 times larger than in common blood. This outcome was relevant to those made by Ehrenfest et al. [21], Eren et al. [22], and Grecu et al. [23]. Besides, PRF had a uniform fibrin network, and cells (platelets and leukocytes) could be trapped in the fibrin structure. As a consequence, our study revealed that the human PRF collection methodology could be applied to mouse PRP preparation.
Regenerative capacity was evaluated by testing PRF for cytotoxicity and cell migration in vitro. mBMCs were tested using the MTT assay, and the results announced that gPRF was a biocompatible material. It also promoted cell migration and increased cell viability compared to serum-free media [24].
The consequences of Asherman syndrome include dysmenorrhea, infertility, and miscarriage because of fibrosis and adhesion in the uterine cavity, which develop as a reaction to injury to the basal endometrium. According to our published protocol, we successfully settled up the murine model of Asherman syndrome in female mice [15]. Following the D0, the uterine structure was damaged by a 25-gauge needle. The regeneration process after injury still occurred; however, after three estrus cycles, adhesions in the uterus were formed. Moreover, this experiment was performed on female mice that had been given a litter of pups to remove the primary infertility issue. In Asherman’s mouse model, gPRF was injected into both uterine horns via the vagina at the di-estrus of the third estrus cycle. The greater the EA/THA, the greater the thickness of the endometrium. In addition, the endometrial gland count as well as the absence of fibrotic adhesions, were recorded when a single dosage of gPRF (20 μL/horn) was administered to the uterine horns. Furthermore, when compared to the untreated mouse, gPRF improved mating results in the mouse model group. The study has shown that the gPRF effectively supports endometrial regeneration by promoting the proliferation of endometrial cells in the uterus [25].
In addition, histological images demonstrated that gPRF played a role in modifying the endometrium’s structure and shape to prepare it for pregnancy. The disappearance of the superficial villi system, the presence of subnuclear vacuoles, and the presence of pseudostratified columnar epithelium in endometrial epithelial cells in the therapy group are morphological indicators of uterine function during pregnancy. This phenomenon is similar to tissue structure in oestrus in vivo [26]. The modification of the plasma membrane in the luminal epithelium has produced deeper tight junctions and fewer lateral connections, which has increased subnuclear vacuoles at or around the time of embryo attachment. The endometrial function is reflected in the occurrence of hypersecretion, altered uterine gland form, and the presence of subnuclear vacuoles. Early secretory phase endometrial glands have been found to be the location of this phenomenon [27]. In addition, several portions displayed sparse gland distribution and muscle adhesions, which are consistent with the clinical and etiological symptoms of human IUA. Furthermore, the negative control group (PBS infusion) showed a considerable decline in gland counts, indicating that the ovarian cycle had not yet fully recovered after injury [2].
The findings suggest that gPRF may be effective for treating Asherman syndrome. The limitations of this study included the small sample size, short treatment time, immunostaining marker of adhesion proteins, and molecular level evaluations required to determine which gPRF elements improve endometrium regeneration and specific mechanisms.
5. CONCLUSION
In this study, gPRF with 5 times the platelet counts of whole blood was injected into uterine horns. In the murine model of Asherman syndrome, using one dose of gPRF (20 μL/horn) for two horns at the diestrus increased the number of uterine glands, the thickness of the endometrium, and the outcome of pregnancy. Furthermore, the underlying mechanism of regeneration of the endometrial epithelium in gPRF should be studied in greater depth in the future.
6. ACKNOWLEDGMENT AND/OR DISCLAIMERS, IF ANY
This study was funded by the Department of Science and Technology, Ho Chi Minh City under grant number 29/2020/H?-QPTKHCN.
7. AUTHORS’ CONTRIBUTIONS
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work. All the authors are eligible to be an author as per the International Committee of Medical Journal Editors requirements/guidelines.
8. CONFLICTS OF INTEREST
The authors report no financial or any other conflicts of interest in this work.
9. ETHICAL APPROVALS
Animal methods in this research were accepted by the ethics committee of the University of Science (580B/KHTN-ACUCUS).
10. DATA AVAILABILITY
All data generated and analyzed are included within this research article.
11. PUBLISHER’S NOTE
This journal remains neutral with regard to jurisdictional claims in published institutional affiliation.
REFERENCES
1. Dreisler E, Kjer JJ. Asherman's syndrome:Current perspectives on diagnosis and management. Int J Womens Health 2019;11:191-8. [CrossRef]
2. Yu D, Wong YM, Cheong Y, Xia E, Li TC. Asherman syndrome-one century later. Fertil Steril 2008;89:759-79. [CrossRef]
3. Senturk LM, Erel CT. Thin endometrium in assisted reproductive technology. Curr Opin Obstet Gynecol 2008;20:221-8. [CrossRef]
4. Azizi R, Aghebati-Maleki L, Nouri M, Marofi F, Negargar S, Yousefi M. Stem cell therapy in Asherman syndrome and thin endometrium:Stem cell-based therapy. Biomed Pharmacother 2018;102:333-43. [CrossRef]
5. Ajwani H, Shetty S, Gopalakrishnan D, Kathariya R, Kulloli A, Dolas R, et al. Comparative evaluation of platelet-rich fibrin biomaterial and open flap debridement in the treatment of two and three wall intrabony defects. J Int Oral Health 2015;7:32-7.
6. Hoaglin DR, Lines GK. Prevention of localized osteitis in mandibular third-molar sites using platelet-rich fibrin. Int J Dent 2013;2013:?80. [CrossRef]
7. Yelamali T, Saikrishna D. Role of platelet rich fibrin and platelet rich plasma in wound healing of extracted third molar sockets:A comparative study. J Maxillofac Oral Surg 2015;14:410-6. [CrossRef]
8. Ehrenfest DM, Andia I, Zumstein MA, Zhang CQ, Pinto NR, Bielecki TJ. Classification of platelet concentrates (Platelet-Rich Plasma-PRP, Platelet-Rich Fibrin-PRF) for topical and infiltrative use in orthopedic and sports medicine:Current consensus, clinical implications and perspectives. Muscles Ligaments Tendons J 2014;4:3-9. [CrossRef]
9. Borie E, OlivíDG, Orsi IA, Garlet K, Weber B, Beltrán V, et al. Platelet-rich fibrin application in dentistry:A literature review. Int J Clin Exp Med 2015;8:7922-9.
10. Ratajczak J, Vangansewinkel T, Gervois P, Merckx G, Hilkens P, Quirynen M, et al. Angiogenic properties of 'leukocyte-and platelet-rich fibrin'. Sci Rep 2018;8:14632. [CrossRef]
11. Zumstein MA, Berger S, Schober M, Boileau P, Nyffeler RW, Horn M, et al. Leukocyte-and platelet-rich fibrin (L-PRF) for long-term delivery of growth factor in rotator cuff repair:Review, preliminary results and future directions. Curr Pharm Biotechnol 2012;13:1196-206. [CrossRef]
12. Su CY, Kuo YP, Tseng YH, Su CH, Burnouf T. In vitro release of growth factors from platelet-rich fibrin (PRF):A proposal to optimize the clinical applications of PRF. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:56-61. [CrossRef]
13. Ji B, Sheng L, Chen G, Guo S, Xie L, Yang B, et al. The combination use of platelet-rich fibrin and treated dentin matrix for tooth root regeneration by cell homing. Tissue Eng Part A 2014;21:26-34. [CrossRef]
14. Baek HS, Yoo JY, Rah DK, Han DW, Lee DH, Kwon OH, et al. Evaluation of the extraction method for the cytotoxicity testing of latex gloves. Yonsei Med J 2005;46:579-83. [CrossRef]
15. Le TT, Lam HM, Tran HL. Efficiency of mechanical force in establishment of Asherman's syndrome mouse models. Eur J Pharm Med Res 2019;6:639-45.
16. Jang HY, Myoung SM, Choe JM, Kim T, Cheon YP, Kim YM, et al. Effects of autologous platelet-rich plasma on regeneration of damaged endometrium in female rats. Yonsei Med J 2017;58:1195-203. [CrossRef]
17. Zhao S, Lu J, Chen Y, Wang Z, Cao J, Dong Y. Exploration of the potential roles of m6A regulators in the uterus in pregnancy and infertility. J Reprod Immunol 2021;146:103341. [CrossRef]
18. Choukroun J, Diss A, Simonpieri A, Girard MO, Schoeffler C, Dohan SL, et al. Platelet-rich fibrin (PRF):A second-generation platelet concentrate. Part IV:Clinical effects on tissue healing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:56-60. [CrossRef]
19. Pavlovic V, Ciric M, Jovanovic V, Stojanovic P. Platelet rich plasma:A short overview of certain bioactive components. Open Med 2016;11:242-7. [CrossRef]
20. Pham TA, Nguyen HT, Nguyen MT, Trinh VN, Tran NY, Ngo LT, et al. Platelet-rich fibrin influences on proliferation and migration of human gingival fibroblasts. Int J Exp Dent Sci 2016;5:83-8. [CrossRef]
21. Ehrenfest DM, Del Corso M, Diss A, Mouhyi J, Charrier JB. Three-dimensional architecture and cell composition of a Choukroun's platelet-rich fibrin clot and membrane. J Periodontol 2010;81:546-55. [CrossRef]
22. Eren G, Gürkan A, Atmaca H, Dönmez A, Atilla G. Effect of centrifugation time on growth factor and MMP release of an experimental platelet-rich fibrin-type product. Platelets 2016;27:427-32. [CrossRef]
23. Grecu AF, Grecu D, Nica O, Ciuca EM, Camen A, Ciurea ME. A novel method of obtaining platelet rich fibrin from rats and quantifying platelet count. Curr Health Sci J 2019;45:104-10.
24. Ehrenfest DM, Doglioli P, Giuseppe M, Del Corso M, Charrier JB. Choukroun's platelet-rich fibrin (PRF) stimulates in vitro proliferation and differentiation of human oral bone mesenchymal stem cell in a dose-dependent way. Arch Oral Biol 2010;55:185-94. [CrossRef]
25. Wang Y, Chen X, Mao L, Cui L, Bai W. Therapeutic effect of platelet-rich fibrin transplant on formation of thin endometrium. Exp Clin Transpl 2021;19:600-8. [CrossRef]
26. Ye X. Uterine luminal epithelium as the transient gateway for embryo implantation. Trends Endocrinol Metab 2020;31:165-80. [CrossRef]
27. Mazur MT, Kurman RJ. Normal endometrium and infertility evaluation. In:Diagnosis of Endometrial Biopsies and Curettings. Berlin, Germany:Springer;2005. 7-33. [CrossRef]