
1. INTRODUCTION
Amenorrhea is the absence of menstruation during the reproductive age in women. Amenorrhea is not a sickness, but rather a symptom, caused by a variety of factors such as pregnancy, prepubertal, POF, menopausal, absence of uterus and vagina, imbalanced hormone, increased amount of male testosterone, endometritis, inappropriate ovarian function, and vaginalagenesis. Menstrual irregularity affects 5% of Indian women, showing that it is a persistent issue for them [1]. In females, regular menstruation is one of the signs of overall health and self-awareness of well-being [2]. As per the World Health Organization (WHO), amenorrhea is considered the sixth most common source accounting for 15% of all infertility in female patients. Amenorrhea is a sign of some unidentified disease that might be in the hypothalamic-pituitary gland-ovaries-uterine axis [3].
Amenorrhea is of two types primary and secondary amenorrhea (SA). The primary amenorrhea (PA) is the absence of a menstrual cycle to occurs in women at the age of 14 years if the secondary sexual characteristics are absent. PA is a symptom that can be caused by various disorders such as endocrinal, hormonal imbalance, gonadal, physiological, and genetic disorders [4]. Amenorrhea can be connected with clinically challenging pathology and patients require lifelong treatment. The primary amenorrhea patients should be examined thoroughly as it impacts both the physical and psychological health of the patient. Untimely diagnosis and intervention are essential to avoid continuing health illness and social consequences.
SA is the absence of menses for more than three cycles continuously, who has had the periods in the past at least one time. SA can also occur in the body due to natural changes, reasons are more likely to be obese, too much exercise, low body fat, stress, anciety, hormonal imbalance, loss or gain of weight in a short duration, etc. The diagnosis of amenorrhea is extensive and can vary from endocrine disorders, chromosomal abnormalities (CAs), psychological conditions, environmental factors, and structural anomalies.
Various studies have been reported from different parts of the world on etiological factors related to PA. The two significant causes reported are Mullerian anomalies and gonadal dysgenesis which varies the frequency in different parts. The Indian studies on this subject also vary in estimation regarding the rate of different etiologies [5]. CAs have been identified as one of the causes of amenorrhea in cytogenetic studies. Indeed, the role of sex CAs in PA has been thoroughly documented throughout the world. Some people with aménorrhea have several CAs including numerical abnormalities such as 45,X, and mosaicism and structural X chromosome abnormalities, including Xp/q duplications or deletions, ring chromosomes, and isochromosomes, in addition to 46,XY associated with a female phenotype [6]. Turner syndrome (TS) is the most common chromosomal disorder. It is, generally, caused by the complete or partial loss of chromosome X and affects around 1 in every 2500 females. Short stature and ovarian insufficiency are characteristic features that occur in >90% of TS patients [7]. The goal of this study is to determine the cytogenetic pattern among amenorrhea patients and how it relates to their phenotype present in the primary and SA in Indian patients. Karyotype identified with translocation, X chromosome deletion, and derivative chromosomes, patients samples are further investigated with FISH and Chromosomal Microarray. Patient samples with a clinical indication for PA and SA with no uterus, blind vagina, streak ovaries, hypoplastic uterus, and minimal clinical history were taken for the study.
2. MATERIALS AND METHODS
The present study was performed on 292 patients samples with a clinical indication who are suspected of the primary and SA. All the total 292 patients are positive amenorrhea patients, who are above the age of 14, we have checked for CA and segregated the normal karyotype and abnormal karyotype. All the samples taken for the study were positive amenorrhea patients, which is confirmed by the clinician and cytogenetic studies performed to find out the positive and negative CAs. Ethical clearance and approval for the study were obtained from the Institutional Bio-safety and Ethics Committee/IRB of Satyabama Institute Science and Technology (Ref-136 IRB-IBSEC/SIST), Chennai, Tamil Nadu, India.
2.1. Sample Collection
The samples were collected from Indian patients from various hospitals and clinics. Clinical indications with USG findings such as blind vagaina, no uterus, infantile uterus, and streak ovaries. Hormonal imbalance with hypothyroidism and phenotype defects with short stature, undeveloped secondary sexual characters, etc., samples was received for cytogenetic analysis. Once the sample is received in the laboratory that each sample has been registered with a unique ID and taken to the laboratory for processing. Our study was carried out with approval from the ethical committee for diagnosis and experiments in human blood samples. From each patient along with the test request form, the signed consent form was also taken as per the rules and regulations of the organizational ethics committee at the time of sample collection. The study involves patients with referred PA (n = 243) and SA (n = 49) for chromosomal analysis (Karyotyping) to the Cytogenetic Laboratory of Lifecell International Pvt. Ltd April 2018–July 2021. Inclusion criteria for sample collection were from 14 to 45 years old patients. Around 2–4 mL of peripheral venous blood were collected aseptically from each patient in a heparinized collection tube to avoid sample contamination.
2.2. Cytogenetic Study
According to the standard cytogenetic protocol, Peripheral blood was collected, cultured, and harvested, and metaphase slides were prepared and stained. Karyotyping analysis was performed by GTG banding technique with trypsin and Giemsa at approximately 400–500 bphs. For each sample, duplicate tubes were performed according to CAP and NABL guidelines. The stained slides were loaded in an automation microscope and the required number of metaphases were selected and performed karyotyping with the ASI software Version 8.0 (Genesis, USA). A minimum of 20 metaphases were analyzed for each patient sample to rule out any CA and 50 cells for mosaicism patients. The report provided is based on the recommendations of (ISCN 2016 and ISCN 2020) as these are retrospective data from 2018 to 2021. Patients identified with structural or numerical CAs were recommended for further treatment and genetic counseling.
3. RESULTS AND DISCUSSION
A total of 292 samples were cultured and analyzed for the study with both primary and SA. Of these, 243 were from PA and 49 were from early SA patients. In PA out of 243 patients, 72.8% (177) were with normal chromosomes, even though few identified with no uterus, hypoplastic uterus, small ovaries, streak gonads, etc., and 27% (66) patients with abnormal karyotype were identified [Figure 1 and Table 1].
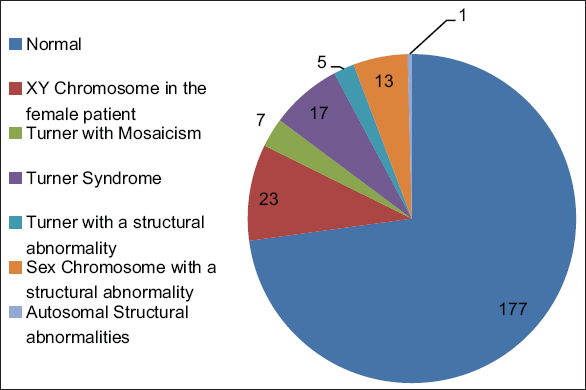 | Figure 1: Cytogenetic findings of the PA patients. [Click here to view] |
Table 1: Karyotype withstructural and numerical abnormalities in PA patients.
| S. No. | Cytogenetic findings | Karyotype | No. of patients | Percentage | USG Findings |
|---|---|---|---|---|---|
| 1. | Normal | 46, XX | 177 | 72.8 | Uterus Absent (12), Hypoplastic (48), Normal Uterus (155) |
| 2. | XY Chromosome in the female patient | 46, XY | 23 | 9.5 | Uterus Absent (5), Hypoplastic (1), Normal Uterus (18) |
| 3. | Turner with Mosaicism | mos 45, X/46, XY | 1 | 0.4 | Uterus Absent (3), Hypoplastic (3), Normal Uterus (27) |
| mos 47, XXX/45, X | 3 | 1.2 | |||
| mos 45, X/46, XX | 3 | 1.2 | |||
| 4. | Turner Syndrome | 45, X | 17 | 7.0 | |
| 5. | Turner with a structural abnormality | mos 45, X/46, X, i (X)(q10) | 5 | 2.1 | |
| 6. | Sex Chromosome with a structural abnormality | 46, X, del (X)(q22) | 1 | 0.4 | Uterus Absent (2), Hypoplastic (3), Normal Uterus (14) |
| 46, X, del (X)(p11) | 1 | 0.4 | |||
| 46, X, i (X)(q10) | 6 | 2.5 | |||
| 45, XX, rob (13;14)(q10;q10) | 1 | 0.4 | |||
| 46, X, iNV dup (X)(q10p22) | 1 | 0.4 | |||
| 46, X, i (X)(q ter ->q10::q10 ->q ter | 2 | 0.8 | |||
| 46, del (X)(q27), dup (X)(q21.3q27.1) | 1 | 0.4 | |||
| 7. | Autosomal Structural abnormalities | 46, XX, t (2;10)(p24;p13) | 1 | 0.4 | Normal Uterus |
In the present study, cytogenetic findings are classified into seven types. They are as follows: (i) Normal female Karyotype: 46,XX with no CA but with PA in 177 patients, (ii) developmental sexual disorder with female phenotype: 46,XY find out in 23 patients [Figure 2b], and (iii) turner with Mosaicism: One patient was with 45,X/46,XY turner with Developmental sexual disorder. Three patients with turner and numerical abnormality (47,XXX/45,X ) and three patients with normal female karyotype and turner (46,XX/45,X) were identified with turner with mosaicism. (iv) Pure Turner: Most observed CA 45,X is the cause of PA, a total ofseventeen patients are found with a turner [Figure 2a]. (v) Turner with Structural abnormality: Totally five patients were karyotyped with mosaic turner with structural abnormality mos 45,X/46,X, i(X)(q10). Sex chromosome with structural abnormality: Thirteen patients are found to have structural abnormality in X chromosome. Out of thirteen, eight patients were identified with isochromosomes [Figure 2f]. In the short and long arm of X chromosome. Deletion in the X chromosome were identified in two patients and one patient identified with Robertsonian translocation [Figure 2d], sex chromosome Inversion duplication identified in one patient[Figure 2e]. Sex chromosome Deletion and duplication in one patient. (vii) Autosomal structural abnormality: one patient was karyotyped with autosomal translocation.
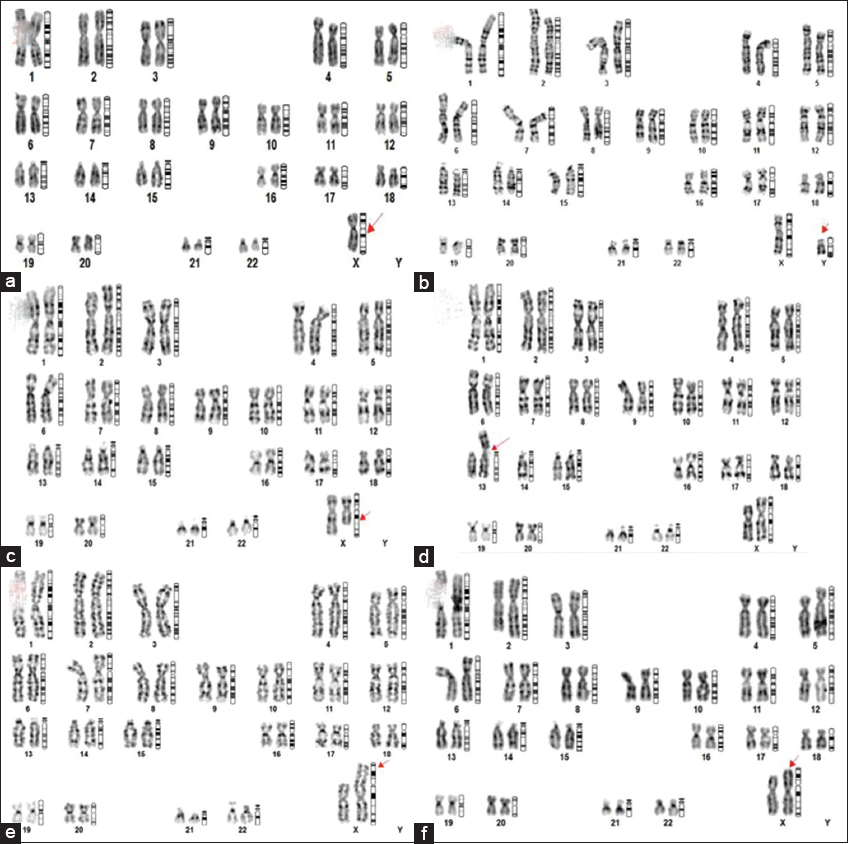 | Figure 2: Chromosomes abnormality (a) 45,X – Turner Syndrome, (b) 46,XY DSD – Abnormal with developmental sexual disorder, (c) 46,X,del(x)(q22) Sex chromosome with deletion, (d) 45,XX,rob (13;14)(q10;q10) Autosomal structural abnormality, (e) 46,X,iNV dup (x)(q10p22) Sex chromosome with inversion and duplication, and (f) 46,X, i(x)(q10) Isochromosome). [Click here to view] |
In SA out of 49 patients, 81.6% were with normal chromosomes and the remaining 18% of patients were karyotyped with a CA, the below are the cytogenetic findings [Table 2]: (i) Normal female karyotype: Forty patients were identified with normal female karyotype, (ii) TS: Only one patient in SA identified with 45,X [Figure 2a], (iii) turner with Mosaicism: Mosaicism with turner and normal female karyotype were identified in one patient, and (iv) sex chromosome with structural abnormality: A total of six patients were identified with sex chromosome structural abnormality, Deletion in X chromosome in three patients [Figure 2c], Derivative X chromosome in one patient, Isochromosome in one patient, and Robertsonian translocation in one patient [Figure 2d]. (v) Turner with structural abnormality: Sex chromosome mosaicism and structural abnormality identified in one patient.
Table 2: Karyotype with structural and numerical abnormalities in SA patients.
| S. No. | Cytogenetic findings | Karyotype | No. of Patients | Percentage |
|---|---|---|---|---|
| 1. | Normal | 46, XX | 40 | 81.6 |
| 2. | Turner syndrome | 45, X | 1 | 2.0 |
| 3. | Turner with mosaicism | mos 45, X/46, XX | 1 | 2.0 |
| 4. | Turner with a structural abnormality | mos 45, X/46, X, del (X)(q22) | 1 | 2.0 |
| 5. | Sex chromosome with a structural abnormality | 46, X, i (X)(q10) | 1 | 2.0 |
| 46, X, del (X)(q25) | 1 | 2.0 | ||
| 46, X, der (X) t(?;X)(?;q27) | 1 | 2.0 | ||
| 46, X, del (X)(q22) | 1 | 2.0 | ||
| 45, XX, rob (13;14)(q10;q10) | 1 | 2.0 | ||
| 46, X, del (X) (P 11.1) | 1 | 2.0 |
Most countries worldwide have been undertaken to study the prevalence of CA in the primary and SA patients. The most fundamental investigation in the diagnosis of amenorrhea is cytogenetic study. Various studies indicate the sex CAs frequency in amenorrhea patients. According to published literature, CAs seem to be one of the most common reasons for PA. The percentage reported ranges from 15.9% to 63.3% with CAs. This massive range of percentages is attributable to differences in the size of the sample as well as patient selection criteria. The chromosomal aberrations identified, out of 490 PA patients were 121 (24.7%) [8]. In the present study, out of 243 PA patients, the CA was identified in 27% (6 6) and SA patients out of 49 (18%) were identified with the CA. In addition, the majority of the instances documented are numerical and structural sex CAs. In India, in most of the rural areas, peoples have no awareness of sex-related defects and diagnosis is less. Hence, the true prevalence of female sex CAs in individuals with amenorrhea is unknown.
Turner’s syndrome (45,X) is one of the most common forms of female gonadal dysgenesis. Clinical symptoms of TS are short stature, broad shield-like chest, nomalous auricles, webbed neck, and hypoestrogenemia resulting in undeveloped sexual characters. Mosaicism occurs in approximately 25% of patients with Turner’s syndrome [9]. According to Vijayalakshmi et al. [10], the major cause of PA is TS. The present study also indicates, the frequency of 45,X and mosaic turner arehigh with 17.9% and different types of mosaic Turner with different karyotypes (45, X/46, XX; 45, X/46, XY; 45X/47,XXX; 45, X/46, X, i(Xq); and 45,X/46,X,del(Xq). Growth hormone treatment is a successful and safe approach to developing growth in TS patients. The second frequent abnormality in PA is 46,XY DSD patients that have different phenotypic characteristics, but the physical manifestation of the DSD could happen later. The present investigation also the percentage of 46,XY DSD is high at 9.5%. Swyer syndrome is associated with a mutation in the SRY gene and as a result, the testes are dysgenetic and do not produce testosterone or anti-Mullerian factor [11]. Although there are various reasons, numerous researchers proved that polycystic ovarian syndrome (POS) is one of the most often genetically identified causes of SA. A few people with POS have been reported to have chromosomal changes, according to certain sources [12]. However, POS could be caused by X chromosomal mutations or translocations. There is a gene (POF1) localized to Xq21.3-q27 or inside Xq26.1-q27 [13,14] and a gene (POF2) localized to Xq13-q21.1.15, according to reports with POF and Xq deletions.
Ovarian failure is also common in Triple X [15]. Therefore, for cytogenetic investigation, individuals with SA should be referred so that chromosome abnormalityis excluded from the study. According to the WHO, 15% of worldwide people are infertile, with amenorrhea being the sixth most common source of women’s infertility. Amenorrhea was found to impact 2–5% of all women of reproductive age in the general population [16]. Amenorrhea’s etiology has been divided into abnormalities of the outflow tract/ovary/anterior pituitary/CNS components, as well as hereditary variables [17]. In the area of medicine, genetic factors are recognized to be “the primary factors” for the majority of illnesses. Similarly, whatever the cause of amenorrhea is the “genetic basis” that must be stressed. Single gene disorders/CAs or multifactorial genetic factors could be involved. Chromosomes and their anomalies are the most common among them, and they all contribute to the constitutional etiology of amenorrhea.
In live births, the frequency of CAs is roughly 90/10,000. The occurrence includes both numerical (monosomy/trisomy/mosaicism) and structural chromosomal aberrations (translocation/isochromosome/deletion/duplication/ring) [18]. The most common structural anomalies that contribute to PA are Isochromosomes of the long arm of X (i[Xq]), [19]. The structurally defective X chromosome could be inactivated, minimizing cellular function disruption.
Furthermore, the size of the deleted or duplicated regions in X, as well as the loss/gain/altered genetic activity, may have an indirect effect on the phenotype. A similar finding was made in the present investigation, where some of our patients had the X qiso chromosome. A wide range of surveys conducted throughout the world to measure the rate of sex chromosomal aberrations in patients having primary or SA has revealed a wide range of chromosomal defects [20,21]. The percentage of CAs identified with 26.13% in the primary and 16.33% in SA patients in a retrospective study of 620 women with primary and 245 women with SA [22]. Aside from numerical and structural X CAs include marker, ring, isochromosomes for long arm, and X autosome translocations. All of these abnormalities were seen in both their pure and mosaicism. There were also other records of reciprocal and Robertsonian translocations.
Although many studies were carried out onamenorrhea patients, the karyotype findings are moreover similar. The rare findings in our study, 21-year-old PA patients witha hypoplastic uterus were karyotyped withinv dup (X) (q10p22). Second rare case identified was with deletion and duplication in the X chromosome. 46,del(X)(q27),dup(X)(q21.3q27.1) in a 17-year-old patient with no pubic and axillary hairs and with a normal uterus. In general, duplications in chromosomes are less harmful than deletions in chromosomes, but they are certainlyassociated with some clinical abnormalities [23]. The third rare finding is mos 47,XXX/45,X in three patients with hypoplasticuterus/normal uterus with poorly developed secondary sexual characters,ages ranging from 17, 21, and 27, respectively.
The CAs observed in our study were with various sex CA with deletion such as 46,X,del(X)(q22) and 46,X,del(X)(p11), Duplication 46,del(X)(q27),dup(X)(q21.3q27.1), Inversion46,X,inv dup (X)(q10p22), and Robertsonian translocation 45,XX,rob(13;14)(q10;q10). Thus, the present research investigation emphasizes the different abnormality in sex chromosomes that highlights not only turner 45,X as the cause of the primary and SA but also other abnormality in sex chromosomes that lead to amenorrhea. While most of the studies state that sex chromosomes are involved in the cause of amenorrhea, but, in our study, few patients identified with Robertsonian translocation showed delayed menarche in patients. To rule out this, extensive history is required for the study. Compared to the primary and SA, the CA is less in SA patients.
USG findings of the patients with hypoblastic/normal/no uterus, normal, and abnormal karyotype were identified. In no uterus patients, the percentage of CA is 54.5% (12) and normal karyotype 45.5% (10); both are almost the same. In hypoplastic uterus patients, the normal karyotypeis 87.3% (48) and CA are 12.7% (7). In comparison with normal and abnormal karyotypes, patients with hypoplastic uterus patients are with normal karyotype. In patients with a normal uterus, the normal karyotypeis 71.4% (155) and CA are 28.6% (62); the CA is identified less in the normal uterus. Patients with the primary and SA, having CAs, are recommended and essential to have genetic counseling along with hormone therapy, and other treatment methods for fertility [24].
There is no medicinal treatment for genetic disorders, and only genetic counseling can be provided to prevent and for further management. After removal of the non-genetic causes by the gynecologists, patients with symptoms or clinical features of PA should be referred for genetic study [25]. The early diagnosis and cytogenetic investigation of amenorrhea will help the patients to know about the genetic makeup and help them to get counseled to understand and manage them in good health.
4. CONCLUSION
CAs are one of the major etiological conditions for PA and SA patients. Person could not able to attain menarche at the age of 14–16 y need to consult the physician to get medical guidance in the early stage. Patients may with any of the symptoms such as mental retardation, PA, SA, short stature, and poorly developed secondary sexual characteristics are recommended to diagnose with cytogenetic analysis. Early diagnosis in SA patients might help to assist and decide on reproduction options. Thus, cytogenetic analysis confirms the diagnosis, a better understanding of the phenotype, and genotype of the patients. CA can also be identified with new techniques like FISH, X inactivation, or more recent technique like chromosomal microarray to rule out the CAs.
5. ACKNOWLEDGMENT
I would like to thank Mr.Mayur Abaya, Managing Director of Life Cell International Pvt. Ltd for funding opportunity and permitting to carry out the study. I also thank all technical staff of the cytogenetic department and Dr.Ambiga Ramesh, PRIST University for guiding me in writing the paper for publication.
6. AUTHORS’ CONTRIBUTIONS
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work. All the authors are eligible to be an author as per the International Committee of Medical Journal Editors (ICMJE) requirements/guidelines.
8. CONFLICTS OF INTEREST
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
9. ETHICAL APPROVALS
Ethical clearance and approval for the study were obtained from the Institutional Bio-safety and Ethics Committee/IRB of Sathyabama Institute Science and Technology (Ref-136 IRB-IBSEC/SIST), Chennai, Tamil Nadu, India.
10. DATA AVAILABILITY
All data generated and analyzed are included in this research article. If any other data supporting this study are available on request.
11. PUBLISHER’S NOTE
This journal remains neutral with regard to jurisdictional claims in published institutional affiliation.
REFERENCES
1. Tanmahasamu P, Rattanachaiyanont M, Dandrat C, Indhavivadhan S, Angsuwattana S, Techatraisak K. Causes of primary amenorrhea:A report of 265 patients in Thailand. J Obstet Gynaecol Res 2012;38:297-301. [CrossRef]
2. David AK, Scott LP, Reeder RM. Amenorrhea:A systematic approach to diagnosis and management. Am Fam Physician 2019;100:39-48.
3. KriplaniA, Goyal M, Kachhawa G, Mahey R, KulshresthaV. Etiology and management of primary amenorrhoea:A study of 102 cases at tertiary centre. Taiwan J Obstet Gynecol 2017;56:761-4. [CrossRef]
4. Ali A, Indriyati R, Winarni T, Faradz S. Cytogenetic analysis and clinical phenotype of primary amenorrhea in Indonesian patients. J Biomed Transl Res 2018;4:22-7. [CrossRef]
5. Mishra RK, Kohli UA, Seth A, Tripathy SR. Etiology of primary amenorrhea:Experience from a tertiary care hospitalin Western India. Med J DY Patil Vidyapeeth 2021;14:674-8. [CrossRef]
6. Dutta UR, Ponnala R, Pidugu VK, Dalal AB. Chromosomal abnormalities in amenorrhea:A retrospective study and review of 637 patients in south India. Arch Iran Med 2013;16:267-70.
7. Li N, Zhao L, Li J, Ding Y, Shen Y, Huang X, et al. Turner syndrome caused by rare complex structural abnormalities involving chromosome X. Exp Ther Med 2017;14:2265-70. [CrossRef]
8. Korgaonkar S, Dhangar S, Kulkarni V, Kerketta L, Vundinti BR. Clinical and cytogenetic profile of 490 patients of primary amenorrhea. J Med Sci Clin Res 2018;6:487-94.
9. Anagani M, Agrawal P, Radhika B, Sridevi D, Karee M. Primary amenorrhea-a one year review. Obstet Gynecol Int J 2017;6:1-4. [CrossRef]
10. Vijayalakshmi J, Koshy T, Kaur H. Cytogenetic analysis of patients with primary amenorrhea. Int J Hum Genet 2010;10:71-6. [CrossRef]
11. Samal R, Habeebullah S. Primary amenorrhea:A clinical review. Int J Reprod Contracept Obstet Gynecol 2017;6:4748-53. [CrossRef]
12. Netter A, Bloch-Michel H, Salmon V, Thervet F, De Grouchy J, Lamy, M. Etude du caryotypedans la maladie de stein Leventhal. Ann Endocrinol 1961;22:241-6.
13. Therman E, Laxova R, Susman B. The critical region on the human Xq. Hum Genet 1990;85:455-61. [CrossRef]
14. Tharapel AT, Anderson KP, Simpson JL, Martens PR, Wilroy RS, Llerena JC, et al. Deletion (X) (q26.1-->q28) in a proband and her mother:Molecular characterization and phenotypic-karyotypic deductions. Am J Hum Genet 1993;52:463-71.
15. Fraaccaro M, Maraschio P, Pasquali F, Scappaticci S. Women heterozy-gous for deficiency of the (p21--->pter) region of the X chromose are fertile. Hum Genet 1977;39:283-92. [CrossRef]
16. World Health Organization 14th Annual Report. Special Programme of Research Development and Research training in Human Reproduction Geneva:World Health Organization;1985. p. 114-9.
17. Speroff L, Glass RH, Kase NG. In:Clinical Gynecologic Endocrinology and Infertility. 6th ed. United States:Lippincott Williams and Wilkins, Amenorrhea;1999. 421-76.
18. Mueller RF, Young ID. Emery's Elements of Medical Genetics. 11th ed. Edinburgh, UK:Churchill Livingstone;2001. 249.
19. Opitz O, Zoll B, Hansmann I, Hinney B. Cytogenetic investigation of 103 patients with primary or secondary amenorrhea. Hum Genet 1982;65:46-7. [CrossRef]
20. Ten SK, Chin YM, Noor PJ, Hassan K. Cytogenetic studies in women with primary amenorrhea. Singapore Med J 1990;31:355-9.
21. Park YS, Kang KC. Cytogenetic study of primary amenorrhea. Korean J Obstet Gynecol 1999;42:814-20.
22. Sayee R, Leelavathy N. Cytogenetic studies in amenorrhea. Saudi Med J 2007;28:187-92.
23. Malla TM, Dar FA, Pandith AA, Zargar MH. Frequency and pattern of cytogenetic alterations in primaryamenorrhea Patients of Kashmir, North India. Egypt J Med Hum Genet 2016;17:25-30. [CrossRef]
24. Afshar H, Najafipour R, Ansari J, Karimi N, Jalilvand M. Cytogenetic analysis in women with primary and secondary amenorrhea in Iran:Retrospective study on 110 patients. J Fundam Appl Sci 2016;8:1173-87. [CrossRef]
25. Pal AK, Ambulkar PS, Sontakke BR, Talhar SS, Bokariya P, Gujar VK. A study on chromosomal analysis of patients with primary amenorrhea. J Hum Reprod Sci 2019;12:29-34. [CrossRef]